
Hospitals need $114 million in quick cash for infrastructure
BRACEBRIDGE — Hospital board chair Evelyn Brown says an immediate $114 million is needed just to keep the Bracebridge and Huntsille sites going in the near future.

In a presentation to the District of Muskoka council recently, she made clear any talk of a single site decision remains years away.
But right now, an instant infusion of infrastructure cash is necessary just to maintain the status quo.
Here’s her presentation below, in a hospital blog she posted.
“The Muskoka Algonquin Healthcare Board of Directors is drawing attention, through our political leaders, to the need for Muskoka ratepayers to start making investments now for future health care capital needs.
On January 19, Phil Matthews, Vice Chair of the Board, and I appeared before the District of Muskoka’s Corporate & Emergency Services Committee to encourage the creation of a reserve fund for health care capital needs. Phil referred to this reserve fund as “a major asset that we don’t have today”.
The timing of our presentation was based on the immediacy of 2018 budget deliberations by the District. The purpose of the presentation was to highlight the capital needs of the health care system and to demonstrate the importance of broad financial support, both today and in the future. Our presentation concentrated on MAHC’s current capital needs and also referenced an order of magnitude for future redevelopment costs.
Our presentation was not for a specific figure or sum of money, but rather was asking consideration be given to creating a health care capital reserve fund supported annually by taxation.
What we know today:
There are significant needs at MAHC today to safeguard and sustain the quality of care we provide. Our presentation indicated that our needs over the next three to five years are estimated at $39 million for equipment, technology and aging building infrastructure. Future redevelopment needs, regardless of the model selected, will be even more substantial (hundreds of millions of dollars over time) and will compound this challenge for our communities.
Currently, there are insufficient funds available to MAHC for replacing capital needs – MAHC relies on the community through donations to our Foundations and Auxiliaries to replace aging infrastructure, and buy new equipment to keep pace with technology. Unfortunately, today’s capital needs outpace community contributions, meaning there are insufficient funds available now to fix aging buildings, let alone to bank toward any future needs.
We also know today that the capital building cost (bricks and mortar) of hospital redevelopment is shared by the Ministry of Health and Long-Term Care, which contributes approximately 90%, and what the Ministry calls the community’s “local share”, which is the remaining 10%. Other infrastructure costs, such as parking lots, new equipment and furnishings, are also expected to be paid for by the community through donations, like they are today. These could add up to an additional 14% or more of the building costs of future redevelopment.
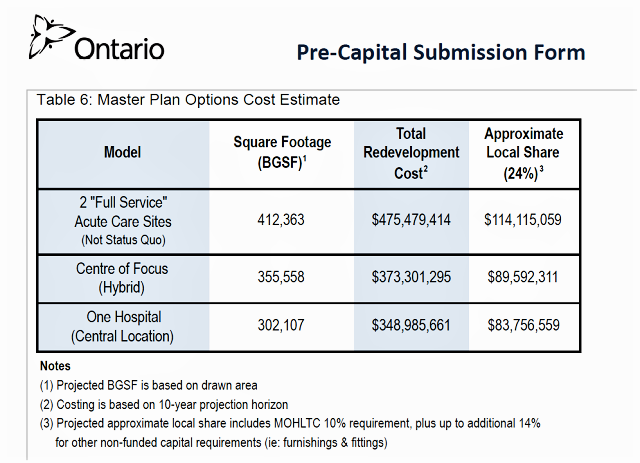
Our presentation referenced the potential order of magnitude of the community share of a future redevelopment. MAHC’s 2015 Pre-Capital Submission to the Ministry of Health and Long-Term Care included the cost surveyors’ estimate of the potential local share plus infrastructure costs of the three models that were previously developed for hospital redevelopment ranging from $84 million to $114 million (shown in the table below).
What we know about the future:
The Capital Plan Development Task Force has been struck by the MAHC Board of Directors to recommend the best model for future hospital care that ensures high-quality, safe and sustainable care for future generations. The task force is committed to a thorough and comprehensive process to look at potential models for the future, even if they are unpopular, to satisfy the requirements of the Ministry of Health and Long-Term Care.
The task force is researching three potential models and developing what programs and services could be provided through each of the models. This process continues and is a new chapter in MAHC’s future planning work and the ending to that chapter has yet to be written. The timeline for the Stage 1 submission is dependent upon doing it right and taking the time that is necessary to ensure appropriate engagement and thorough analysis.
No decisions have been made about the preferred model of delivering acute care in the future.
The task force is aiming to bring its recommendation of a preferred model to the MAHC Board of Directors this spring, and to submit the Stage 1 (Part A & B) to Capital Investment Branch of Ministry by the end of 2018.
Most importantly, we know that regardless of the model recommended by the task force and selected by the Board, it is prudent for Muskoka to begin investing in this multi-million-dollar fund now. Quite simply we can start to incrementally put aside funds now, or massively pay later.
By asking our local leaders for prudence and forethought for the Muskoka ratepayers to support the needs of the health care system today and in the future, we do not believe we are undermining the Stage 1 future planning work that is underway. We are helping our local leaders to understand the role the community will need to play in building the future health care system.”